
Follow Kritica on Google
Add Kritica to your favourite sources.
“Shall I leave the cutter with you?” asks the operator at the hospital triage, where I arrived by ambulance, which I had called myself. I had started cutting my wrists in front of the PC with a small, retractable blue cloud-shaped craft knife. I have been under the care of my city's Mental Health Centre (CSM) for four years. Four years of medication, four years of seeing a psychiatrist, with a six-month gap during the transition from my old psychiatrist to the new one. Six months of nothing. Six months of swallowing medication alone.
In four years of CSM, I have earned an exemption from the ticket for “Major Depression – recurrent episodes”. But this is not enough to gain access to psychoanalysis or, more generally, to psychotherapy, which is nevertheless highly recommended by every psychiatrist who has seen me.
The nurse then took the cutter, deeming her colleague's opinion of leaving it with me inappropriate after he had told me that these things aren't done, that there are people who care about me who would be hurt by my action, that everything can be resolved. All things he was saying in good faith, candid and well-intentioned in his paternalism and his total unawareness of the situation.
According to the Ministry of Health’s 2024 Report, 845,516 people received mental health care in 2024. 55.9% of these were women. “With regard to depression in particular,” the Report states, “the proportion of female service users is almost double that of male service users.” Now, a quick glance at the figures for staff working in care facilities makes it clear just how much we miss Basaglia and his entire theory.
“The total number of staff within public psychiatric units in 2024 stands at 33,142. Of these, 14.5% are doctors (psychiatrists or other specialisms), and 7.0% are psychologists”.
The 7% from a psychologist’s perspective.
We are almost 60 million inhabitants in Italy. 10,732 units means that for every psychologist there are potentially 5,000 or more users.
The Report continues. For example, regarding Psychiatric Diagnosis and Treatment Services (SPDC): “In 2024, the number of active SPDCs is 307 with a total of 3,762 beds for ordinary admissions and 298 beds for admissions in Day hospital; The affiliated healthcare facilities providing psychiatric care number 19, with a total of 543 beds for ordinary hospitalisation and 13 for day hospital. For Italy as a whole, the provision for ordinary hospital beds is 9.2 per 100,000 adult inhabitants.
No further comments are needed.
May has just ended, Mental Health Awareness Month. This month marks the anniversary of the so-called Basaglia law, Law 180 of 13 May 1978. With this law, Italy, the first internationally, closed down asylums.
Up until that moment, the prevailing law, known as the Giolitti law, stipulated that patients were deprived of their civil rights and registered in the criminal record, effectively losing the ability to self-determine and make their own decisions. Asylums were, in practical reality, prisons, places of true confinement, even physical restraint, with measures of containment and shock.
Not only that: the asylum was not exclusively a facility for people with psychiatric conditions; there were also individuals with alcohol addiction, Down's syndrome, people with disabilities, or simply the destitute. In short, people locked up there because society had no place for them. Because outside they were dangerous, scandalous, and unproductive (in the capitalist sense of the term, of course).
“Abele's Gardens” by Sergio Zavoli, is a memorable report which, 10 years before Law 180, documents the situation of patients in the Gorizia mental hospital, their living conditions and Franco Basaglia’s work towards a form of care that did not involve the marginalisation and destruction of the individual.
The voice-over reminds us: “After all, when and why does the madman become socially questionable and dangerous? At the end of the 16th century, when the practical prerequisite of the Borgeoisie society, which was beginning its rise to power, required the marginalisation of unproductive elements in order to rationalise production.”.
This is a key point in the story, because it inextricably links mental distress to social distress and to a specific economic and political system that imposes on individuals a life that is literally inhuman, dictated by the demands of profit.
“Perhaps I'm not ill,” says one of the patients, with extreme and disarming lucidity. "Well, it’s easy to be accepted by people on the outside; you just need money, don't you? [...] To be understood, you have to talk about work [...] Even an ill person has easy relationships with others when they're working, when they're seen to be working and making money, then they're considered by society. Society asks me to be a man, to produce [...] If I talk about films, the sun, poetry, etcetera, nobody listens to me, whereas if I talk about serious things, about money, everyone listens to me.".
Under the Mariotti Act of 1968, patients regained their civil rights. Furthermore, the Act set a maximum number of beds in care facilities, thereby preventing overcrowding.
Basaglia understands something else: he creates artistic workshops and cooperatives of working patients, so that patients can have a salary and gain dignity and autonomy, escaping that poverty which often caused their internment or, in any case, compounded their illness.
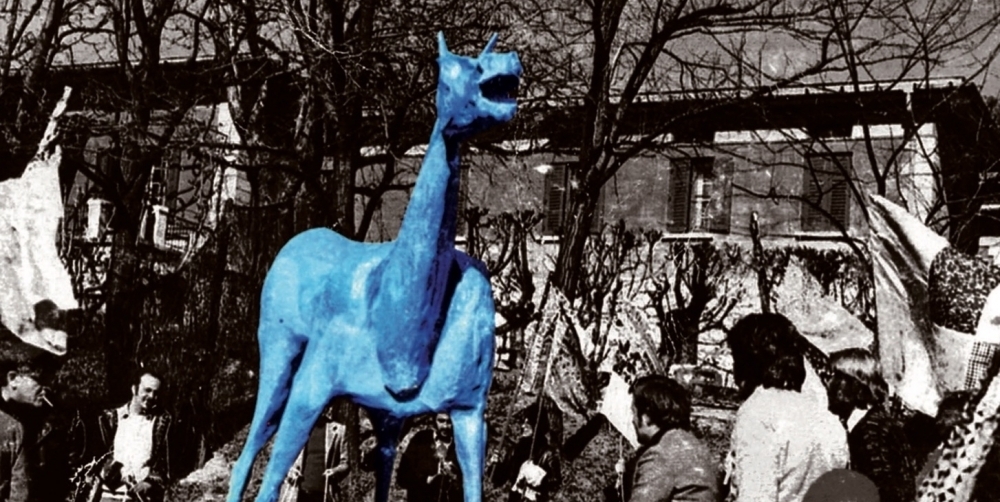
In the wake of these revolutionary actions, the movement “Democratic Psychiatry” was born in 1973. Marco Cavallo it is the name of the work created in 1973 by a group of artists: Vittorio Basaglia and Giuliano Scabia, Federico Velludo, Ortensia Mele, Stefano Stradiotto. Created together with the institutionalised patients. A blue horse (as they wished) around 4 metres high which symbolically crossed the threshold of the asylum to free all that imprisoned humanity.
The closure of asylums presumed the creation of a system of community-based services.
Exactly in the same year, the National Health Service is born.
Italy was a country at the forefront.
He was.
However, from that moment to the present day, a new form of closure has been established. The regions deliver services through Mental Health Departments, which, however, are perpetually understaffed, do not receive sufficient funding, and are unable to meet the needs of the population.
In my town, Pomezia in the province of Rome, to give an example, there is just one CSM. Within this CSM, there are only two “permanent” psychologists. A single CSM serving a population of over 60,000. Not to mention those in the neighbouring municipality of Ardea (almost 50,000).
48 years after the Basaglia Law was enacted, throughout Italy there is a lack of resources, facilities, and staff.
While the colleague of the operator who wanted to leave me the scalpel with the little blue cloud finally puts it in their pocket, I'm in a state of semi-sleep, waiting on the blue triage armchair.
I'm being moved on a stretcher. I’m in the inner area of the Emergency Department. And I remain there for hours, with blood coagulating on my wrists and my shirt stained red. I stay there, in a very convenient spot to see all the other patients, predominantly elderly, who come in complaining of pain, calling the nurses, moaning, screaming. In my head it's total chaos, I wish I could switch everything off but I don't know how.
At one point, I see a patient being brought in with a gun on his belt. He's a guard, perhaps he works there. He's feeling unwell, they lay him on a stretcher, he's unconscious. I stare at him intently. I keep thinking about the weapon within reach. I don't have a box cutter, but there's something more effective there. I stop a nurse who's rushing past, and who replies irritably. I ask if there's any news of the psychiatrist who's supposed to see me. She's not from that ward, she doesn't know, I have to ask the A&E nurse, the ones who dart here and there like grasshoppers because the staff are always too few to cope with everything that comes in from outside. I stop the right nurse. A moment and she arrives. I ask about the psychiatrist, she replies that she doesn't know, that he's been informed, but he has a ward to manage, so he's very busy. She's about to leave, but I hold her back: I tell her about that man, the one with the gun; I tell her that my head is telling me to go over there and take that gun.
Magic happens. Suddenly, two psychiatrists from the ward appear. They are there with me, they ask me questions, they are kind, they recommend I be admitted. Initially, I don't want to, but then I agree. They inject me with benzodiazepines and I fall asleep. They wake me up when it's time to take me to the ward.
My flatmate is a kind and cheerful lady: “You know how I would live if I didn't have this burden? Like a butterfly”. I arrive already dazed, a nurse gets me something to eat (they didn't give me dinner in A&E), I eat, but I don't remember everything that happens afterwards very well. They definitely give me my medication and then drops to help me sleep. And I sleep, I sleep a dreamless sleep. And the next day I continue to sleep, I do nothing but sleep. “The induced sleep is so deep that it leaves no dream traces, but it doesn't restore”., so writes Andrea Pomella in one of his posts throughout his hospital stay that he shared on Facebook. Medication is the main therapy in these places. Indeed, perhaps the only therapy.
I'm looking at the weekly activity schedule. I notice that individual psychological counselling is never scheduled. Never. Every morning there's a medical visit, focused on adjusting medication dosages. But never individual psychological counselling. There are group activities, though. Optional. I'm participating in today's activity.
I believe it's run by a Psychiatric Rehabilitation Therapist. I'm expecting a moment of listening and exchange, of sharing and mutual help. I witness a sort of corporate-style presentation, a PowerPoint document on the notion of “recovery”; a brief initial moment of embarrassment because, before the word appeared on the screen, we had all understood it would be about “admissions”. In short, a series of slides that scroll by, talking to us about recovery paths, identifying resources and tools, and above all about objectives, whether big or small, because objectives give a sense of purpose and determination, they offer the possibility of improving quality of life, they provide that sense of purpose and meaning that makes you feel good and helps you cope better with stress.
Objectives, aims, tools, stress.
Zavoli's documentary comes back to me.
And another thing Pomella writes in her diary: «The doctor tells me a story, one day in the car she found herself stuck in a traffic jam, after a while a cyclist overtakes her, behind him he has a sign that says: ’You're not stuck in traffic, you are the traffic“, she looks at me with tender, shining eyes: ”Do you understand what I mean?‘’
One of the girls in the group will try to harm herself and will therefore be sedated and tied to the bed. One of the boys will punch the wall so hard that he injures himself; he will then be sedated and rendered completely harmless: a zombie who mumbles and drools. Another boy sleeps constantly, without stopping; he doesn’t speak, eats his meals and goes back to sleep. We gather in a small group to protest against this crisis management and to ask why the activity plan does not include a regular one-to-one session with the psychologist. The ward manager arrives and makes a joke about the fact that we’re gathered as if at a trade union meeting, then says candidly that, should it be necessary, we can request a consultation with the psychologist. Should it be necessary. I reply, “Excuse me, but in a psychiatric ward, who doesn’t need regular one-to-one sessions with a psychologist?” I also add that Basaglia hasn’t even set foot in here. She throws up her hands and exclaims, “Oh, Basaglia…”. I conclude by saying that I will sign to be discharged against medical advice.
In front of the doctor on duty, I say everything that’s on my mind, including my view that certain group therapies – which it takes a great deal of courage to even call ‘therapies’ – are pointless. I mention Franco Basaglia’s name once again, met with a pair of furrowed brows that seem unaccustomed to dealing with adult, sentient, thinking beings.
They infantilise us. In the psychiatric ward, patients aren't really people, or at least not people on an equal footing with doctors and nurses. They're like children, who need to be managed, treated. I got the same impression in the A&E department regarding the elderly: in that case too, non-persons da gestire, anche con un certo fastidio. Perché la vecchiaia è terribile, la vecchiaia urla, sbava, si fa la pipì addosso.
Nel suo diario a un certo punto Pomella dice al medico che “se penso alle cose da fare una volta fuori di qui mi viene voglia di trasformarmi in un albero, in una ringhiera di ferro battuto, in un cartello che indica l’uscita d’emergenza”. Ho avuto esattamente lo stesso pensiero. Intendo l’albero. Ho pensato che avrei voluto trasformarmi in un albero, anche perché nell’unico spazio aperto a noi concesso non c’era nemmeno una piantina, nemmeno una macchia di verde. C’era una palla un po’ sgonfia con una faccia disegnata sopra e un nome: Wilson.
Anche nel diario di Pomella appare questo personaggio, che forse esiste spesso nei servizi dedicati alla salute mentale: “Ieri camminando in giardino mi sono fermato a fissare il moncone di un ramo segato di netto, qualcuno con della vernice rossa ci ha disegnato sopra due occhi e una bocca sorridente, un rametto di tuia cresciuto lì accanto ha coronato lo smile con un ciuffo di capelli, ho pensato che potrebbe chiamarsi Wilson, come il pallone di Tom Hanks”.
Wilson è l’unico confidente di Tom Hanks nei panni del protagonista di Cast Away, l’unico essere con cui può parlare, confidarsi, sfogarsi, sopra un’isola sperduta. Nel reparto siamo noi piccole isole inascoltate. A volte scambiamo qualche parola, si intesse qualche tipo di legame, ma non è un parlare profondo, un affondo nel nascosto dell’inconscio che possa farci almeno tentare un percorso di guarigione. La psicoterapia non è prevista in reparto, e non è prevista nemmeno nei CSM, saturi di pazienti e scarsi di personale. Le liste di attesa sono infinite, quindi per molti la psicoterapia resta un miraggio e si va avanti solo con i farmaci. Oppure si decide di fare ulteriori sacrifici e rivolgersi a un privato.
Io, nel frattempo, contro il parere medico, esco da un reparto psichiatrico in cui la grande maggioranza di ospiti è giovane, di quella gioventù che dovrebbe mangiarsi le piazze e le strade, invece di stare chiusa in una prigione a dormire, angosciarsi e odiarsi.
C’è una ragazza felicissima di uscire. Andrà in clinica. Conosco purtroppo certe procedure. So che spesso, dopo il SPDC c’è la clinica o la comunità, che non è più totalmente sovvenzionata dal SSN, ma convenzionata o totalmente privata. Ho un’amica che si trova in comunità da tre anni ormai e quando ascolto i suoi messaggi vocali non la riconosco quasi più, non capisco cosa mi dice, biascica, è rallentata, è annientata dai farmaci.
La questione della salute mentale è una questione complessa, che oltrepassa i confini della medicina e della psicologia. Lo sguardo deve andare più lontano, proprio lì dove arrivava Franco Basaglia, al tessuto sociale in cui il “malato” deve (re)inserirsi. Un individuo per stare bene ha bisogno di un posto nella società, nella comunità degli esseri umani, e per averlo ha bisogno di un’autonomia, che ad oggi è data dal lavoro. Far parte della comunità dei lavoratori permette una presa di coscienza: permette di capire che il disagio psichico è legato a doppio filo con quello sociale; permette di capire che si hanno dei diritti, che vanno rivendicati a gran voce.
“Tu devi essere partecipe”, scrivo a B., giovanissima ospite del mio stesso SPDC. Devono riunirsi per decidere del suo futuro e io spero che riesca a esprimere chiaramente i suoi bisogni e a rivendicare i suoi diritti. Questo sistema tende a mettere a tacere, a sedare con i farmaci le falle di una struttura sociale che ormai non regge più. I farmaci possono attenuare i sintomi di un malessere, ma la radice del male non è esclusivamente dentro l’individuo. È un intreccio complesso fra il dentro e il fuori. Se il fuori è un sistema capitalistico e guerrafondaio disumanizzante, spersonalizzante, in cui la persona è sacrificata al profitto, alla produttività gestita insensatamente in direzione di guadagni sempre maggiori per i pochi padroni della terra, allora il terreno di azione è molto più ampio dei confini di una singola mente.
© Kritica – Riproduzione consentita solo parzialmente (non più di metà articolo) inserendo il link e la fonte all’inizio.
